
THE TRADITIONAL CONCEPT OF THE SURGERY
OF THE VARICOSE VEINS IS CALLED INTO QUESTION
The traditional concept considers that the saphenous vein is the first affected (dilation and backward flow), and thus that it is at the origin of the varicose disease. The evolution is described from top to bottom: the disease develops from the termination of the saphenous vein (with the inguinal fold for the great saphenous vein and with the popliteal fossa for the small saphenous vein), progresses on by the saphenous trunk on the thigh then on the calf, up to the peripheral collaterals on which the varicose veins develop. According to the traditional theory, the responsibility for the saphenous vein in the development of the varicose veins leads to the systematic ablation of this one to treat the problem in a “radical” way. This principle has been applied since 1907, date on which an American surgeon (W.W. Babcock) described the technique of the treatment of the varicose veins by ablation of the saphenous vein. This principle remains the same one, nearly 100 years afterwards.
Several elements led us to wonder about this traditional conception of the responsibility for the saphenous vein, and about the corollary principle of the systematic ablation of the saphenous vein:
> the frequency of the repetitions of varicose veins after the ablation of the saphenous vein (30 to 70% according to studies); how to explain that the varicose veins return whereas the saphenous vein was removed?;
> the existence of the patients who present varicose veins without their saphenous vein being affected; would these patients, often young, be at the early stage of the disease?;
> the existence of only one type of intervention (the ablation of the saphenous vein by stripping) whatever the age, symptoms and localization of the varicose veins; in spite of a case of figure often particular to each patient, would it exist only one type of surgical operation for the varicose veins?
A.S.V.A.L. METHOD:
A NEW PHYSIOPATHOLOGICAL CONCEPT
The A.S.V.A.L. method is based on a concept opposite to the traditional concept, the ascending evolution of the varicose disease starting from the peripheral veins, from bottom to upwards: the smallest and superficial veins, whose wall is most fragile, would be the first to be dilated (heredity, traumatism, pregnancy, ageing…). The evolution would remain initially in the subcutaneous plan near the skin, creating a superficial venous network dilated and flowing back. This flowing back superficial network would end up creating an aspiration effect in the saphenous vein (located in the major subcutaneous plan), generating a backward flow initially reversible. The saphenous vein is the superficial vein of which the wall is the thickest, protected in addition by the unfolding of the subcutaneous fascia in which it progresses. This is why it will be the last to be degraded.
A.S.V.A.L. METHOD:
A NEW THERAPEUTIC APPROACH
The physiopathological conception of the A.S.V.A.L. method led to preserve the saphenous vein, with two principles:
1/ The early treatment of the varicose veins to protect the saphenous vein as long as it is not flowing back.
2/ The ablation of the varicose veins without ablation of the saphenous vein, even flowing back. Recent studies show that the saphenous vein recovers a satisfactory operation in 91% of the cases after the ablation of the varicose veins. The ablation of the saphenous vein would be indicated only in the situations where the attack of the saphenous vein seems irreversible.
The preservation of the saphenous vein has several interests:
• Physiological: even if it is known that the saphenous vein drains only 10% of the totality of the venous blood of the lower limb, it has certainly a major role for the subcutaneous drainage.
• Anatomical: the great saphenous vein is used for the realization of bypass heart or peripheral operations on the lower limbs. In certain cases, no other material than the vein of the patient can be used to carry out a bypass operation.
The idea of the A.S.V.A.L. method is thus a selective management of the superficial venous backward flows, according to the clinical and haemodynamic context suitable for the situation of each patient.
A.S.V.A.L. METHOD:
LESS AGGRESSIVE TECHNIQUES - SIMPLER CONTINUATIONS
1/ Softer Surgery:
All the surgical gestures of the A.S.V.A.L. method are guided by the respect of tissues. The ablation of collateral varicoses is made by meticulous phlebectomy with the hook according to the technique described by Müller. The principle is to withdraw the longest possible segment of vein through several incisions, without rupture, to decrease the bleeding. The incisions of phlebectomy are micro-incisions, of less than two millimetres. Generally, all the gestures are as atraumatic as possible, in particular during the handling of the hooks. That requires that the gestures are precise, from there the importance of the location by a rigorous preoperative cartography.
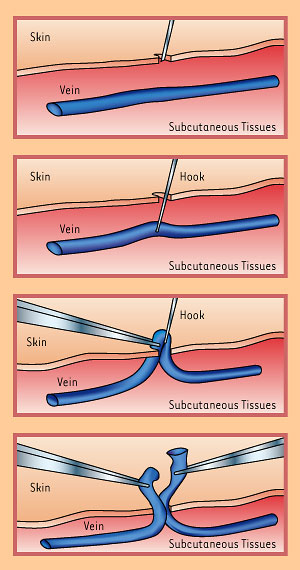
Phlebectomy: after having made a micro-incision,
the surgeon can reach the sick vein which it makes go up using a tiny hook.
The vein is seized with grips, is divided and withdrawn.
The gesture is very delicate and respects the subcutaneous skin and tissues.
2/ Lighter anaesthesia:
Except exceptional case, the anaesthesia always purely local, is very diluted. This mode of anaesthesia has several advantages: reduction of the anaesthetic risk, major reduction of the operational bleeding (thus of the postoperative ecchymoses and haematomas) by effect of vasospasm, early ambulation (thus prevention of venous thrombosis and lesser disability).
3/ Simpler continuations:
The patient can leave one hour after the end of the intervention, and it is advised to him to walk as much as possible. No activity is formally prohibited in the days which follow, apart from prolonged trampling, a long sitting travel or an intensive sport.
The studies show that the use of these less aggressive surgical and anaesthetic techniques reduce in a very important way the postoperative pains (42% of the patients do not take any antalgic treatment and 86% less than six tablets in the first eight postoperative days) and the duration of the interruption of work (7 days on average, but 25% of the patients work on the following day).
A.S.V.A.L. AND C.H.I.V.A.
The Haemodynamic Cure of the Venous Insufficiency in Ambulatory (C.H.I.V.A.) is also opposed to the ablation of the saphenous vein, but without calling into question the responsibility for the saphenous vein in the appearance of the varicose veins. Indeed, it has as a principle to redistribute the superficial venous flow of the surface (varicose veins and saphenous vein) towards the depth (deep venous trunks), by using a system of shunts on the saphenous circuit and the perforating veins, by a surgical operation which segments the surface backward flow, with staged tyings.
The A.S.V.A.L. and the C.H.I.V.A. methods are thus basically different: for the A.S.V.A.L. the saphenous vein can “be cured” by the ablation of the varicose veins, whereas for the C.H.I.V.A. the saphenous vein can be used to drain the varicose veins towards the deep veins.
A.S.V.A.L. AND ENDOVEINOUS LASER
The endoveinous laser makes it possible to destroy the saphenous vein by heat. It claims to replace the surgical ablation of the saphenous vein (stripping) by a less aggressive method. The physiopathological concept of the endoveinous laser is the same one as that of the traditional surgery: it is the saphenous vein which is responsible for the varicose disease and it is thus the one that should be removed. The treatment by endoveinous laser is thus in opposition with the A.S.V.A.L. method whose principle is to preserve the saphenous vein as far as possible. Moreover the endoveinous laser does not remove the varicose veins, which will be treated by phlebectomies with the hook (thus surgical operation) or sclerotherapy, in the same time or after the laser session.